



开放科学(资源服务)标识码(OSID): 
颊黏膜癌是常见的口腔肿瘤之一,其发病率在不同国家和地区差异较大[1,2]。在南亚地区颊黏膜癌尤为高发,仅次于舌癌[3]。在我国,口腔癌症的发病率约为48.1/10万,而颊黏膜鳞癌占口腔癌的20.8%~37%[2,4]。颊黏膜癌的病理类型包括鳞状细胞癌、腺癌、黏液表皮样癌等,其中鳞癌是其最常见的病理类型[5]。颊黏膜癌的侵袭性强,预后差,其生存率低于口腔其他位置的肿瘤,5年生存率仅为44.10%[2]。既往研究表明婚姻状态与多种癌症的生存显著相关,如肺癌、乳腺癌、胃癌、胰腺癌等[6]。颊黏膜鳞癌已明确的独立预后危险因素有:年龄、病理类型、分化程度、手术和美国癌症联合委员会(American Joint Committee on Cancer, AJCC) 癌症分期等[7,8]。然而,婚姻状态对颊黏膜鳞癌患者生存的影响尚不明确。本文从权威肿瘤数据库——美国国立癌症研究所“监测、流行病学和结果” (surveillance, epidemiology, and end results, SEER)数据库获取18个肿瘤注册点的数据[9,10],进行多中心回顾性研究,探究婚姻状态对颊黏膜鳞癌患者生存的影响,为颊黏膜鳞癌患者的风险评估、护理及临床决策提供科学依据。
1 资料和方法
1.1 病例来源和筛选
1.2 一般资料
本研究提取到患者的一般资料如下:婚姻状态、种族、性别、诊断年龄、诊断年份、分化程度、AJCC分期、手术以及生存状态和随访时间。根据患者的婚姻状态,本研究将患者分为3组:已婚、未婚和不良婚姻,其中不良婚姻包括离异、分居和丧偶。随访时间为从确诊到死亡或随访截止(2015年12月31日)的时间。
1.3 统计学分析
使用SPSS 25.0软件进行统计学分析,定性资料比较用卡方检验。采用Kaplan-Meier分析和Log-rank检验初步探究婚姻状态对颊黏膜鳞癌患者生存的影响。通过单因素和多因素COX比例风险回归分析校正其他因素对婚姻状态预后作用的混杂影响。P < 0.05为差异有统计学意义。
2 结 果
2.1 患者的基本资料
本研究共纳入1 006例颊黏膜鳞癌患者,其中已婚567例(56.4%)、未婚173例(17.2%)和不良婚姻266例(26.4%)。已婚组、未婚组、不良婚姻组在诊断年龄、性别、人种、AJCC分期、是否手术中差异有统计学意义(P<0.05);而诊断年份和分化程度的差异无统计学意义(P>0.05)。见表1。
表1 1 006例颊黏膜鳞癌患者的基本资料
Table 1
| Variables | Married | Never married | Unhappily married | χ2 | P |
|---|---|---|---|---|---|
| Age at diagnosis | |||||
| ≤ 60 years | 222(62.4) | 98(27.5) | 36(10.1) | 93.275 | < 0.001 |
| >60 years | 345(53.1) | 75(11.5) | 230(35.4) | ||
| Sex | |||||
| Male | 388(67.0) | 109(18.8) | 82(14.2) | 107.341 | < 0.001 |
| Female | 179(41.9) | 64(15.0) | 184(43.1) | ||
| Race | |||||
| White | 428(55.1) | 130(16.7) | 219(28.2) | 51.880 | < 0.001 |
| Black | 22(30.1) | 28(38.4) | 23(31.5) | ||
| Others* | 117(75.0) | 15(9.6) | 24(15.4) | ||
| Year of diagnosis | |||||
| 2004-2009 | 227(55.4) | 74(18.0) | 109(26.6) | 0.419 | 0.811 |
| 2010-2015 | 340(57.0) | 99(16.6) | 157(26.3) | ||
| Grade | |||||
| Hight | 455(54.8) | 151(18.2) | 224(27.0) | 5.275 | 0.072 |
| Low | 112(63.6) | 22(12.5) | 42(23.9) | ||
| AJCC stage | |||||
| Ⅰ | 151(63.4) | 27(11.3) | 60(25.2) | 15.033 | 0.020 |
| Ⅱ | 123(56.2) | 38(17.4) | 58(26.5) | ||
| Ⅲ | 102(56.7) | 26(14.4) | 52(28.9) | ||
| Ⅳ | 191(51.8) | 82(22.2) | 96(26.1) | ||
| Surgery | |||||
| No evidence | 71(39.7) | 42(23.5) | 66(36.9) | 24.702 | < 0.001 |
| Yes | 496(60.0) | 131(15.8) | 200(24.2) | ||
| Total | 567(56.4) | 173(17.2) | 266(26.4) | - | |
*:Others includes American Indian/Alaska Native and Asian/Pacific Islander
2.2 婚姻对颊黏膜鳞癌患者生存的影响
如图1所示,已婚患者的生存最好,不良婚姻的患者生存最差(P<0.001),已婚的中位生存时间为59个月,未婚的中位生存时间为26个月,而不良婚姻的中位生存时间为20个月。如表2所示,单因素分析显示,婚姻状态、诊断年龄、性别、AJCC分期、分化程度以及手术均对颊黏膜鳞癌患者的生存有影响(P<0.05)。通过多因素COX比例风险回归校正诊断年龄、性别、AJCC分期、分化程度以及手术的混杂影响,结果表明婚姻状态是颊黏膜鳞癌患者预后的独立危险因素(P=0.001)。已婚患者的生存最佳,与之相比,未婚患者的死亡风险高29.7%(校正后HR=1.297,P=0.040),不良婚姻患者的生存最差,死亡风险比已婚患者高44.5%(校正后HR=1.445,P=0.001)。
图1
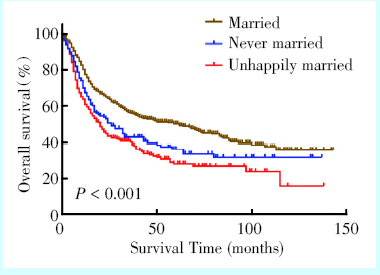
图1
婚姻状态对颊黏膜鳞癌患者的生存分析
Figure 1
Survival analysis of marital status on patients with buccal mucosa squamous cell carcinoma
2.3 不同诊断年龄下各婚姻状态的生存分析
如图2a~b所示,无论在低龄组(≤ 60岁)还是高龄组(>60岁),婚姻状态均对颊黏膜鳞癌患者的生存有影响。其中,在低龄组和高龄组中,已婚患者的生存均比未婚和不良婚姻患者的更佳(P < 0.05)。
2.4 不同AJCC分期下各婚姻状态的生存分析
如图2c~f所示,AJCC分期Ⅰ、Ⅲ、Ⅳ期中,已婚患者的生存均比未婚和不良婚姻患者的更佳(P <0.05)。而在Ⅱ期中,与未婚和不良婚姻患者相比,已婚患者的生存虽然也呈现出较好的趋势,但差异不具有统计学意义(P=0.125)。
3 讨 论
3.1 婚姻影响颊黏膜鳞癌患者的生存
本研究在单因素和多因素分析中均发现已婚患者的生存优于未婚和不良婚姻患者,明确了婚姻状态对颊黏膜鳞癌患者的预后具有独立作用。在不同年龄组与不同的AJCC分期中也观察到,婚姻状态可影响颊黏膜鳞癌患者的生存。Aizer 等[6]通过734 889肿瘤病例分析婚姻状态对患者生存的影响,发现与未婚和不良婚姻患者相比,已婚患者的死亡率更低。Gao等[12]研究也发现,婚姻状态是软骨肉瘤患者预后的独立危险因素,与已婚患者相比,未婚、离婚和丧偶患者的生存更差,死亡率更高。此外,在AJCC分期Ⅱ期的亚组分析中,与已婚患者相比,未婚患者和不良婚姻患者的生存呈现更差的趋势,但不具有统计学差异。此结果与Gao等[12]研究结果类似,在分期亚组分析中,对于局限期的患者,婚姻状态对软骨肉瘤患者生存影响不具有统计学意义。张倩等[13]探究婚姻对肺癌生存的影响时也发现,在高分化组,婚姻状态对肺癌患者的生存影响无统计学意义。这具体原因尚不清楚,可能与亚组分析样本量较低有关,需要进一步探究。
Table 2 Univariate and multivariate analyses of prognostic factors in patients with buccal squamous cell carcinoma
| Variables | Univariate analysis | Multivariate analysis | ||
|---|---|---|---|---|
| HR (95% CI) | P | HR (95% CI) | P | |
| Marital status | < 0.001 | 0.001 | ||
| Married | 1 | 1 | ||
| Never married | 1.439(1.137-1.822) | 0.003 | 1.297(1.012-1.661) | 0.040 |
| Unhappily married | 1.751(1.439-2.132) | < 0.001 | 1.445(1.173-1.780) | 0.001 |
| Age at diagnosis | < 0.001 | < 0.001 | ||
| ≤ 60 years | 1 | 1 | ||
| >60 years | 1.634(1.347-1.983) | < 0.001 | 1.640(1.330-2.023) | < 0.001 |
| Sex | 0.011 | 0.908 | ||
| Male | 1 | 1 | ||
| Female | 1.251(1.052-1.489) | 0.011 | 1.011(0.839-1.218) | |
| Race | 0.081 | – | ||
| White | 1 | |||
| Black | 1.223(0896-1.669) | 0.206 | ||
| Others* | 0.799(0.616-1.036) | 0.091 | ||
| Year of diagnosis | 0.218 | – | ||
| 2004-2009 | 1 | |||
| 2010-2015 | 0.893(0.747-1.069) | 0.218 | ||
| Grade | < 0.001 | 0.017 | ||
| Hight | 1 | 1 | ||
| Low | 1.563(1.266-1.929) | < 0.001 | 1.302(1.049-1.615) | 0.017 |
| AJCC stage | < 0.001 | < 0.001 | ||
| Ⅰ | 1 | 1 | ||
| Ⅱ | 1.312(0.961-1.790) | 0.087 | 1.152(0.843-1.574) | 0.374 |
| Ⅲ | 2.023(1.488-2.750) | < 0.001 | 1.713(1.255-2.338) | 0.001 |
| Ⅳ | 4.100(3.165-5.310) | < 0.001 | 3.281(2.507-4.294) | < 0.001 |
| Surgery | < 0.001 | < 0.001 | ||
| No evidence | 1 | 1 | ||
| Yes | 0.223(0.183-0.271) | < 0.001 | 0.331(0.270-0.407) | < 0.001 |
*:Others includes American Indian/Alaska Native and Asian/Pacific Islander
图2
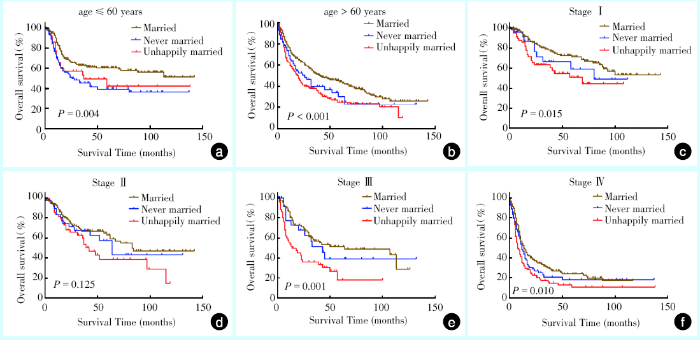
图2
颊黏膜鳞癌患者不同诊断年龄与AJCC分期下各婚姻状态的生存分析
Figure 2
Survival analysis of marital status of buccal squamous cell carcinoma at different diagnostic ages and AJCC stages
a: survival analysis of marital status at diagnostic age ≤ 60 years, b: survival analysis of marital status at diagnostic age > 60 years; c:survival analysis for marital status based on stage Ⅰ; d: survival analysis for marital status based on stage Ⅱ; e: survival analysis for marital status based on stage Ⅲ; f: survival analysis for marital status based on stage Ⅳ
3.2 未婚和不良婚姻患者生存更差的原因分析
4 小 结
在护理和临床实践中,除了要关注颊黏膜鳞癌患者传统的肿瘤生物学特征,还需要关注患者的婚姻状态。尤其对于未婚患者和不良婚姻患者,注重对这部分患者的宣教,加强对其心理社会支持,关注患者的心理健康,并积极随访增强患者的依从性;对于已婚的患者,除了加强患者的关注,还要提醒配偶多给予患者精神心理支持以及监督好患者的依从性。本研究存在一定的局限性:①本研究的病例来源于美国的SEER数据库,患者以白人为主,与我国的文化背景不一致,研究结果不一定能完全反映本国患者的情况;②SEER数据库只记录了诊断时的婚姻状态,不能评估婚姻状态变化对颊黏膜鳞癌患者生存的影响;③SEER数据库缺失了患者婚姻质量的信息,不能进一步评估婚姻质量对生存的影响。下一步的研究应纳入我国的病例,收集患者婚姻质量,进一步评估婚姻质量对颊黏膜鳞癌患者生存的影响。

参考文献
Buccal space tumours
[J].
OBJECTIVE: To review the available literature as it pertains to the buccal space with a specific focus on the pathologies encountered within this space. Clinical presentation, investigations, and surgical approaches to the region are also reviewed. METHODS: A systematic review of the available literature was performed on buccal space tumours from 1980 to 2017. Data was extracted on clinical presentation, investigations and surgical approaches to the buccal space. The pathologies encountered in the buccal space were reviewed and presented. RESULTS: Forty-nine unique articles were reviewed, with a total 217 patients. The age of the patients ranged from 0 to 83 with a mean age of 45.8. A total of 51 pathologies were reported. The majority of these were vascular and salivary gland pathologies. The majority of salivary gland neoplasms were malignant. However a wide variety of benign and malignant soft tissue tumours were also reported to occur in this region. CONCLUSIONS: The buccal space is a small and complex region with a variety of pathologies occurring within it. This review clarifies the differential diagnosis of a mass which presents in this area and the pathologies which occur within it.
Does buccal cancer have worse prognosis than other oral cavity cancers?
[J].
Objectives/Hypothesis: To determine whether buccal squamous cell carcinoma has worse overall survival (OS) and disease-specific survival (DSS) than cancers in the rest of the oral cavity.
Study Design: Retrospective analysis of a large population database.
Methods: We began with a Kaplan-Meier analysis of OS and DSS for buccal versus nonbuccal tumors with unmatched data, followed by an analysis of cases matched for race, age at diagnosis, stage at diagnosis, and treatment modality. This was supported by a univariate Cox regression comparing buccal cancer to nonbuccal cancer, followed by a multivariate Cox regression that included all significant variables studied.
Results: With unmatched data, buccal cancer had significantly lesser OS and DSS values than cancers in the rest of the oral cavity (P<.001). After case matching, the differences between OS and DSS for buccal cancer versus nonbuccal oral cancer were no longer significant. Univariate Cox regression models with respect to OS and DSS showed a significant difference between buccal cancer and nonbuccal cancer. However, with multivariate analysis, buccal hazard ratios for OS and DSS were not significant.
Conclusions: With the largest series of buccal carcinoma to date, our study concludes that the OS and DSS of buccal cancer are similar to those of cancers in other oral cavity sites once age at diagnosis, tumor stage, treatment, and race are taken into consideration. The previously perceived poor prognosis of buccal carcinoma may be due to variations in tumor presentation, such as later stage and older patient age.
Oral cancer: a multicenter study
[J].BACKGROUND: To determine the prevalence and clinicopathologic features of the oral cancer patients. MATERIAL AND METHODS: Biopsy records of the participating institutions were reviewed for oral cancer cases diagnosed from 2005 to 2014. Demographic data and site of the lesions were collected. Sites of the lesion were subdivided into lip, tongue, floor of the mouth, gingiva, alveolar mucosa, palate, buccal/labial mucosa, maxilla and mandible. Oral cancer was subdivided into 7 categories: epithelial tumors, salivary gland tumors, hematologic tumors, bone tumors, mesenchymal tumors, odontogenic tumors, and others. Data were analyzed by descriptive statistics using SPSS software version 17.0. RESULTS: Of the 474,851 accessioned cases, 6,151 cases (1.30%) were diagnosed in the category of oral cancer. The mean age of the patients was 58.37+/-15.77 years. A total of 4,238 cases (68.90%) were diagnosed in males, whereas 1911 cases (31.07%) were diagnosed in females. The male-to-female ratio was 2.22:1. The sites of predilection for oral cancer were tongue, labial/buccal mucosa, gingiva, palate, and alveolar mucosa, respectively. The three most common oral cancer in the descending order of frequency were squamous cell carcinoma, non-Hodgkin lymphoma and mucoepidermoid carcinoma. CONCLUSIONS: Although the prevalence of oral cancer is not high compared to other entities, oral cancer pose significant mortality and morbidity in the patients, especially when discovered late in the course of the disease. This study highlights some anatomical locations where oral cancers are frequently encountered. As a result, clinicians should pay attention to not only teeth, but oral mucosa especially in the high prevalence area as well since early detection of precancerous lesions or cancers in the early stage increase the chance of patient being cured and greatly reduce the mortality and morbidity. This study also shows some differences between pediatric and elderly oral cancer patients as well as between Asian and non-Asian oral cancer patients.
1 751例口腔黏膜鳞癌的构成比分析
[J].
Composition ratio analysis of 1751 cases of oral squamous cell carcinoma
[J].
Oral diseases: a global public health challenge
[J].Oral diseases are among the most prevalent diseases globally and have serious health and economic burdens, greatly reducing quality of life for those affected. The most prevalent and consequential oral diseases globally are dental caries (tooth decay), periodontal disease, tooth loss, and cancers of the lips and oral cavity. In this first of two papers in a Series on oral health, we describe the scope of the global oral disease epidemic, its origins in terms of social and commercial determinants, and its costs in terms of population wellbeing and societal impact. Although oral diseases are largely preventable, they persist with high prevalence, reflecting widespread social and economic inequalities and inadequate funding for prevention and treatment, particularly in low-income and middle-income countries (LMICs). As with most non-communicable diseases (NCDs), oral conditions are chronic and strongly socially patterned. Children living in poverty, socially marginalised groups, and older people are the most affected by oral diseases, and have poor access to dental care. In many LMICs, oral diseases remain largely untreated because the treatment costs exceed available resources. The personal consequences of chronic untreated oral diseases are often severe and can include unremitting pain, sepsis, reduced quality of life, lost school days, disruption to family life, and decreased work productivity. The costs of treating oral diseases impose large economic burdens to families and health-care systems. Oral diseases are undoubtedly a global public health problem, with particular concern over their rising prevalence in many LMICs linked to wider social, economic, and commercial changes. By describing the extent and consequences of oral diseases, their social and commercial determinants, and their ongoing neglect in global health policy, we aim to highlight the urgent need to address oral diseases among other NCDs as a global health priority.
McCarthy EP, et al. Marital status and survival in patients with cancer
[J].
Purpose;To examine the impact of marital status on stage at diagnosis, use of definitive therapy, and cancer-specific mortality among each of the 10 leading causes of cancer-related death in the United States.
Methods;We used the Surveillance, Epidemiology and End Results program to identify 1,260,898 patients diagnosed in 2004 through 2008 with lung, colorectal, breast, pancreatic, prostate, liver/intrahepatic bile duct, non-Hodgkin lymphoma, head/neck, ovarian, or esophageal cancer. We used multivariable logistic and Cox regression to analyze the 734,889 patients who had clinical and follow-up information available.
Results;Married patients were less likely to present with metastatic disease (adjusted odds ratio [ OR], 0.83; 95% CI, 0.82 to 0.84; P < .001), more likely to receive definitive therapy (adjusted OR, 1.53; 95% CI, 1.51 to 1.56; P < .001), and less likely to die as a result of their cancer after adjusting for demographics, stage, and treatment (adjusted hazard ratio, 0.80; 95% CI, 0.79 to 0.81; P < .001) than unmarried patients. These associations remained significant when each individual cancer was analyzed (P < .05 for all end points for each malignancy). The benefit associated with marriage was greater in males than females for all outcome measures analyzed (P < .001 in all cases). For prostate, breast, colorectal, esophageal, and head/neck cancers, the survival benefit associated with marriage was larger than the published survival benefit of chemotherapy.
Conclusion;Even after adjusting for known confounders, unmarried patients are at significantly higher risk of presentation with metastatic cancer, undertreatment, and death resulting from their cancer. This study highlights the potentially significant impact that social support can have on cancer detection, treatment, and survival. (C) 2013 by American Society of Clinical Oncology
Squamous cell carcinoma of tongue and buccal mucosa: clinico-pathologically different entities
[J].The objective of this study was to examine the clinical and pathological features of squamous cell carcinoma of the Tongue and Buccal Mucosa and understand their differences. This is a retrospective analysis of prospectively collected data of 735 patients with squamous cell carcinoma of the tongue and 665 cases of carcinoma of the buccal mucosa treated by surgery at our hospital. Statistical analysis was done to examine clinical and pathological differences between carcinoma of the tongue and the buccal mucosa with regards to age, gender, clinical T stage/N stage, pathological T stage/N stage, overall stage, grade, thickness, perinodal extension (PNE), lymphovascular emboli (LVE) and perineural invasion (PNI). Statistically significant differences were found for factors like age (p < 0.001), gender (p < 0.001), clinical T staging (p < 0.001) and pathological stage (p < 0.001), grade of tumor (p < 0.001) and perineural invasion (p < 0.001) between carcinoma of the tongue and the buccal mucosa. Forty-eight percent patients in either subsite had pathologically proven node negative necks (pN0, p = 0.88). Multivariate analysis for occult nodal metastases revealed that predictive factors were different for the two subsites. There are significant differences between cancers of the tongue and buccal mucosa for various clinical and pathological factors. This may be a reflection of the underlying differences in their causation and pathophysiology. Squamous cell carcinoma in these two subsites should therefore be regarded as clinico-pathologically distinct entities.
Prognostic factors in patients with buccal squamous cell carcinoma: 10-year experience
[J].PURPOSE: Squamous cell carcinoma (SCC) of the buccal mucosa accounts for 23% to 37% of all intraoral cancer cases in Taiwan. Because of the high recurrence rate and invasive tumor behavior, the prognosis is generally poor. The aim of this study was to evaluate the prognostic significance of clinicopathologic factors on survival rates for patients with buccal SCC in a medical center in central Taiwan. MATERIALS AND METHODS: Between March 1995 and December 2002, patients admitted to hospital and diagnosed as having buccal SCC were enrolled in the study. There were 415 patients (406 men and 9 women) 25 to 84 years old (mean age, 51.1 +/- 11.4 years). The chart records were retrospectively reviewed. Relevant clinical features in each patient, such as primary tumor size, tumor stage, initial treatment modalities, surgical margin status, cervical nodal metastasis status, and histopathologic grade, were compared for survival analysis. RESULTS: Three hundred ninety-four patients received surgical intervention. Univariate analysis of relevant prognostic factors showed that positive surgical margin, positive cervical nodal metastasis, positive extracapsular spread, larger tumor, and advanced tumor stage were associated with poor prognosis. Multivariate analysis identified the factors that independently influenced the survival rate as advanced stage disease (stage III: relative risk [RR], 3.09; P = .006; stage IV: RR, 4.64; P < .001), positive surgical margin (RR, 2.02; P = .001), and extracapsular spread of cervical lymph node metastasis (RR, 6.89; P < .001). CONCLUSIONS: This study represents the largest series in the literature and highlights the importance of tumor stage, surgical margin status, and extracapsular spread of cervical nodal metastasis as the most important prognostic factors in patients with buccal SCC.
Cardiovascular disease mortality after chemotherapy or surgery for testicular nonseminoma: a population-based study
[J].PURPOSE: Increased risks of incident cardiovascular disease (CVD) in patients with testicular cancer (TC) given chemotherapy in European studies were largely restricted to long-term survivors and included patients from the 1960s. Few population-based investigations have quantified CVD mortality during, shortly after, and for two decades after TC diagnosis in the era of cisplatin-based chemotherapy. PATIENTS AND METHODS: Standardized mortality ratios (SMRs) for CVD and absolute excess risks (AERs; number of excess deaths per 10,000 person-years) were calculated for 15,006 patients with testicular nonseminoma reported to the population-based Surveillance, Epidemiology, and End Results program (1980 to 2010) who initially received chemotherapy (n=6,909) or surgery (n=8,097) without radiotherapy and accrued 60,065 and 81,227 person-years of follow-up, respectively. Multivariable modeling evaluated effects of age, treatment, extent of disease, and other factors on CVD mortality. RESULTS: Significantly increased CVD mortality occurred after chemotherapy (SMR, 1.36; 95% CI, 1.03 to 1.78; n=54) but not surgery (SMR, 0.81; 95% CI, 0.60 to 1.07; n=50). Significant excess deaths after chemotherapy were restricted to the first year after TC diagnosis (SMR, 5.31; AER, 13.90; n=11) and included cerebrovascular disease (SMR, 21.72; AER, 7.43; n=5) and heart disease (SMR, 3.45; AER, 6.64; n=6). In multivariable analyses, increased CVD mortality after chemotherapy was confined to the first year after TC diagnosis (hazard ratio, 4.86; 95% CI, 1.25 to 32.08); distant disease (P<.05) and older age at diagnosis (P<.01) were independent risk factors. CONCLUSION: This is the first population-based study, to our knowledge, to quantify short- and long-term CVD mortality after TC diagnosis. The increased short-term risk of CVD deaths should be further explored in analytic studies that enumerate incident events and can serve to develop comprehensive evidence-based approaches for risk stratification and application of preventive and interventional efforts.
A population-based study of cardiovascular disease mortality risk in US cancer patients
[J].AIMS: This observational study characterized cardiovascular disease (CVD) mortality risk for multiple cancer sites, with respect to the following: (i) continuous calendar year, (ii) age at diagnosis, and (iii) follow-up time after diagnosis. METHODS AND RESULTS: The Surveillance, Epidemiology, and End Results program was used to compare the US general population to 3 234 256 US cancer survivors (1973-2012). Standardized mortality ratios (SMRs) were calculated using coded cause of death from CVDs (heart disease, hypertension, cerebrovascular disease, atherosclerosis, and aortic aneurysm/dissection). Analyses were adjusted by age, race, and sex. Among 28 cancer types, 1 228 328 patients (38.0%) died from cancer and 365 689 patients (11.3%) died from CVDs. Among CVDs, 76.3% of deaths were due to heart disease. In eight cancer sites, CVD mortality risk surpassed index-cancer mortality risk in at least one calendar year. Cardiovascular disease mortality risk was highest in survivors diagnosed at <35 years of age. Further, CVD mortality risk is highest (SMR 3.93, 95% confidence interval 3.89-3.97) within the first year after cancer diagnosis, and CVD mortality risk remains elevated throughout follow-up compared to the general population. CONCLUSION: The majority of deaths from CVD occur in patients diagnosed with breast, prostate, or bladder cancer. We observed that from the point of cancer diagnosis forward into survivorship cancer patients (all sites) are at elevated risk of dying from CVDs compared to the general US population. In endometrial cancer, the first year after diagnosis poses a very high risk of dying from CVDs, supporting early involvement of cardiologists in such patients.
Characteristics and survival of malignant cardiac tumors: a 40-year analysis of >500 patients
[J].BACKGROUND: The aim of this study was to investigate the incidence, histopathology, demographics, and survival associated with primary malignant cardiac tumors (PMCTs). METHODS AND RESULTS: We queried the Surveillance, Epidemiology and End Results (SEER) 18 registry from the National Cancer Institute for all PMCTs diagnosed from 1973 to 2011. We describe PMCT histopathology and incidence, comparing characteristics and survival of these patients with those of patients with extracardiac malignancies of similar histopathology. From a total of 7 384 580 cases of cancer registered in SEER, we identified 551 PMCTs (0.008%). The incidence of PMCT diagnosis is 34 cases per 100 million persons and has increased over time (25.1 in 1973-1989, 30.2 in 1990-1999, and 46.6 in 2000-2011). Most patients are female (54.1%) and white (78.6%) with median age at diagnosis of 50 years. The most common PMCTs are sarcomas (n=357, 64.8%), followed by lymphomas (n=150, 27%) and mesotheliomas (n=44, 8%). Most patients are diagnosed with tissue sample (96.8%). Although use of chemotherapy is not documented in SEER, 19% of patients received radiation and 44% had surgery. After a median follow-up of 80 months, 413 patients had died. The 1-, 3-, and 5-year survival rates were 46%, 22%, and 17% and have improved over the eras, with 1-, 3-, and 5-year survival rates of 32%, 17%, and 14% for 1973 to 1989 and 50%, 24%, and 19% for 2000 to 2011 (P=0.009). Cardiac sarcomas and mesotheliomas are the most lethal PMCTs, with 1-, 3-, 5-year survival rates of 47%, 16%, and 11% and of 51%, 26%, and 23% compared with 59%, 41%, and 34% for lymphomas, respectively (log rank test P<0.001). Patients with cardiac lymphomas and sarcomas are younger and have worse survival than patients with extracardiac disease of similar histopathology (P<0.001). CONCLUSIONS: PMCTs are extremely rare and continue to be associated with poor prognosis. Over the past 5 decades, the incidence and survival of patients diagnosed with PMCT appear to have increased. Compared with those with extracardiac cancers of similar histopathology, patients with PMCTs are often younger and have worse survival.
Marital status and survival of patients with chondrosarcoma: a population-based analysis
[J].
婚姻状态对肺癌患者生存预后的影响——基于SEER数据库的研究
[J].
Effect of marital status on survival of lung cancer patients investigated based on SEER Database
[J].
婚姻状态对结直肠神经内分泌肿瘤患者远期预后的影响
[J].
Influence of marital status on overall and cancer-specific mortality in patients with colorectal neuroendocrine neoplasm
[J].
The influence of marital status on the use of breast, cervical, and colorectal cancer screening
[J].
The prevalence of psychiatric disorders among cancer patients
[J].Two hundred fifteen randomly accessed cancer patients who were new admissions to three collaborating cancer centers were examined for the presence of formal psychiatric disorder. Each patient was assessed in a common protocol via a psychiatric interview and standardized psychological tests. The American Psychiatric Association's DSM-III diagnostic system was used in making the diagnoses. Results indicated that 47% of the patients received a DSM-III diagnosis, with 44% being diagnosed as manifesting a clinical syndrome and 3% with personality disorders. Approximately 68% of the psychiatric diagnoses consisted of adjustment disorders, with 13% representing major affective disorders (depression). The remaining diagnoses were split among organic mental disorders (8%), personality disorders (7%), and anxiety disorders (4%). Approximately 85% of those patients with a positive psychiatric condition were experiencing a disorder with depression or anxiety as the central symptom. The large majority of conditions were judged to represent highly treatable disorders.
Receipt of psychosocial care among cancer survivors in the United States
[J].
Purpose;Given the importance of psychosocial care for cancer survivors, this study used population-based data to characterize survivors who reported a discussion with health care provider(s) about the psychosocial effects of cancer and who reported using professional counseling or support groups (PCSG) and tested associations between receipt of psychosocial care and satisfaction with care.
Patients and Methods;We examined survivors of adult cancers from the 2010 National Health Interview Survey (N = 1,777). Multivariable logistic regression models examined factors associated with receipt of and satisfaction with psychosocial care.
Results;Most survivors (55.1%) reported neither provider discussions nor use of PCSG; 31.4% reported provider discussion only, 4.4% reported use of PCSG only, and 8.9% reported both. Non-Hispanic blacks (v non-Hispanic whites), married survivors, survivors of breast cancer (v prostate or less prevalent cancers), those treated with chemotherapy, and survivors reporting past research study/clinical trial participation were more likely to report provider discussion(s) (P < .01). Hispanics (v non-Hispanic whites), survivors age 40 to 49 years (v <= 39 years), survivors of breast cancer (v melanoma or less prevalent cancers), those diagnosed <= 1 year ago (v > 5 years ago), survivors treated with radiation, and past research participants were more likely to report use of PCSG (P < .05). Survivors reporting any psychosocial care were more likely to be "very satisfied" with how their needs were met (P < .001).
Conclusion;Many survivors do not report a discussion with providers about the psychosocial effects of cancer, which reflects a missed opportunity to connect survivors to psychosocial services. These data can benchmark the success of efforts to improve access to cancer-related psychosocial care. (c) 2013 by American Society of Clinical Oncology
Baseline utilization of breast radiotherapy before institution of the medicare practice quality reporting initiative
[J].PURPOSE: In 2007, Medicare implemented the Physician Quality Reporting Initiative (PQRI), which provides financial incentives to physicians who report their performance on certain quality measures. PQRI measure #74 recommends radiotherapy for patients treated with conservative surgery (CS) for invasive breast cancer. As a first step in evaluating the potential impact of this measure, we assessed baseline use of radiotherapy among women diagnosed with invasive breast cancer before implementation of PQRI. METHODS AND MATERIALS: Using the SEER-Medicare data set, we identified women aged 66-70 diagnosed with invasive breast cancer and treated with CS between 2000 and 2002. Treatment with radiotherapy was determined using SEER and claims data. Multivariate logistic regression tested whether receipt of radiotherapy varied significantly across clinical, pathologic, and treatment covariates. RESULTS: Of 3,674 patients, 94% (3,445) received radiotherapy. In adjusted analysis, the presence of comorbid illness (odds ratio [OR] 1.69; 95% confidence interval [CI], 1.19-2.42) and unmarried marital status were associated with omission of radiotherapy (OR 1.65; 95% CI, 1.22-2.20). In contrast, receipt of chemotherapy was protective against omission of radiotherapy (OR 0.25; 95% CI, 0.16-0.38). Race and geographic region did not correlate with radiotherapy utilization. CONCLUSIONS: Utilization of radiotherapy following CS was high for patients treated before institution of PQRI, suggesting that at most 6% of patients could benefit from measure #74. Further research is needed to determine whether institution of PQRI will affect radiotherapy utilization.
Early discontinuation and nonadherence to adjuvant hormonal therapy in a cohort of 8,769 early-stage breast cancer patients
[J].PURPOSE: While studies have found that adjuvant hormonal therapy for hormone-sensitive breast cancer (BC) dramatically reduces recurrence and mortality, adherence to medications is suboptimal. We investigated the rates and predictors of early discontinuation and nonadherence to hormonal therapy in patients enrolled in Kaiser Permanente of Northern California health system. PATIENTS AND METHODS: We identified women diagnosed with hormone-sensitive stage I-III BC from 1996 to 2007 and used automated pharmacy records to identify hormonal therapy prescriptions and dates of refill. We used Cox proportional hazards regression models to analyze factors associated with early discontinuation and nonadherence (medication possession ratio < 80%) of hormonal therapy. RESULTS: We identified 8,769 patients with BC who met our eligibility criteria and who filled at least one prescription for tamoxifen (43%), aromatase inhibitors (26%), or both (30%) within 1 year of diagnosis. Younger or older age, lumpectomy (v mastectomy), and comorbidities were associated with earlier discontinuation, while Asian race, being married, earlier year at diagnosis, receipt of chemotherapy or radiotherapy, and longer prescription refill interval were associated with completion of 4.5 years of therapy. Of those who continued therapy, similar factors were associated with full adherence. Women age younger than 40 years had the highest risk of discontinuation (hazard ratio, 1.51; 95% CI, 1.23 to 1.85). By 4.5 years, 32% discontinued therapy, and of those who continued, 72% were fully adherent. CONCLUSION: Only 49% of patients with BC took adjuvant hormonal therapy for the full duration at the optimal schedule. Younger women are at high risk of nonadherence. Interventions to improve adherence and continuation of hormonal therapy are needed, especially for younger women.



{kind=link}
{kind=link}
{kind=link}
{kind=link}